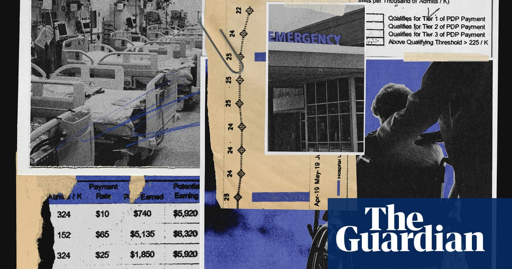
A Guardian investigation finds insurer quietly paid facilities that helped it gain Medicare enrollees and reduce hospitalizations. Whistleblowers allege harm to residents
This shit is complicated because nursing homes do often call EMS unnecessarily(this is where the term GOMER or get out of my emergency room comes from in the first place, someone with acute on chronic conditions who needs to be managed but who inpatient care won’t really improve). Overall these programs aren’t what I’d consider secret and they’re not much different than Medicare giving penalties for readmissions regardless of cause(a policy from the government, not private insurance). But I’m not calling a fucking insurance company or even a provider before EMS if I, as an RN, find stroke symptoms. The standard of care just doesn’t support it and it opens me up to liability. I call EMS and then call the provider, then coordinate care , document, and give report. The last item on that list is calling an insurance company. This is beyond the pale:
In one patient case identified by the Guardian, nursing home staff sent a resident to the hospital because she was found unresponsive, drooling and with a “slant to the side” – possible stroke symptoms. She was admitted to the intensive care unit for a brain bleed, according to a UnitedHealth email reviewed by the Guardian.
But after the incident, instead of praising the facility team for the prompt hospitalization, a UnitedHealth manager alerted her subordinates that the facility team had bypassed the company’s protocol, failing to contact UnitedHealth’s remote on-call team first to receive guidance.
The manager met with the nursing home’s director of nursing services, and scheduled training to re-educate the facility’s nurses, the email shows.
What makes all of this particularly strange is that more than likely the standing orders and policies and procedures of the nursing homes themselves likely maintain the steps I’ve laid out.
It matters because they control both groups involved in this decision and are financially incentivizing not calling a hospital. They aren’t solving how to make a more efficient determination, they’re pushing people away from getting potentially much needed care. They are functionally paying people to not act when lives are on the line. Train them. Teach them. Don’t literally reward them for rolling the dice with lives.
That is a terrible way to incentivize someone to change their behavior when they could be very well determining who lives or dies. And as we gleaned from the article, there have been totally avoidable casualties from this program.
“No one is truly investigating when a patient suffers harm. Absolutely no one,” said one current UnitedHealth nurse practitioner who recently filed a congressional complaint about the nursing home program. “These incidents are hidden, downplayed and minimized. The sense is: ‘Well, they’re medically frail, and no one lives for ever.’”
It’s not complicated. The problem is complicated, but the solution is simple and cruel.
This shit is complicated because nursing homes do often call EMS unnecessarily(this is where the term GOMER or get out of my emergency room comes from in the first place, someone with acute on chronic conditions who needs to be managed but who inpatient care won’t really improve). Overall these programs aren’t what I’d consider secret and they’re not much different than Medicare giving penalties for readmissions regardless of cause(a policy from the government, not private insurance). But I’m not calling a fucking insurance company or even a provider before EMS if I, as an RN, find stroke symptoms. The standard of care just doesn’t support it and it opens me up to liability. I call EMS and then call the provider, then coordinate care , document, and give report. The last item on that list is calling an insurance company. This is beyond the pale:
What makes all of this particularly strange is that more than likely the standing orders and policies and procedures of the nursing homes themselves likely maintain the steps I’ve laid out.
It matters because they control both groups involved in this decision and are financially incentivizing not calling a hospital. They aren’t solving how to make a more efficient determination, they’re pushing people away from getting potentially much needed care. They are functionally paying people to not act when lives are on the line. Train them. Teach them. Don’t literally reward them for rolling the dice with lives.
That is a terrible way to incentivize someone to change their behavior when they could be very well determining who lives or dies. And as we gleaned from the article, there have been totally avoidable casualties from this program.
It’s not complicated. The problem is complicated, but the solution is simple and cruel.